Updated 3/2017-- all links (except to my own posts) removed
as many no longer active. and it was easier than checking each one.
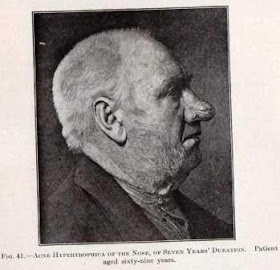
Flipping through the 1908 textbook A Text-Book of Minor Surgery by Edward Milton Foote, MD the photos accompanying the acne hypertrophica section caught my eye. Allow me to share that section of the book with you.
Acne Hypertrophica
This is an overgrowth of the nose, which is generally considered to be one of the forms of acne rosacea, but is here included with the tumors to which it belongs clinically, for the appearance of the lesion and the treatment warrant this classification.This is a disease of middle life, or later, marked by a great overgrowth of the sebaceous follicles, with thier ducts, as well as of blood-vessels and fatty tissue. The skin itself is not greatly thickened, and may even be thinned, apparently the result of over-stretching it. The tumor as a whole is soft and flabby, of dark red color, due to the venous congestion. It is not necessarily the result of alcoholism, and many of these patients are unjustly accused of intemperate habits.Lesser degrees of hypertrophic acne of the nose are frequently found. Such an extreme overgrowth as is shown in Figs 42 and 43 is decidedly exceptional, although even more marked instances are occasionally seen.
Although this overgrowth is benign in character, the excess tissue should be removed, as this can be accomplished without much risk, and the feelings of the patient will thereby be spared many mortifying remarks.
Today we tend to call this problem rhinophyma which is a descriptive term derived from the Greek "rhis" meaning nose and "phyma" meaning growth.
Treatment:
This consists in the removal of wedge-shaped pieces of the growth, so that the normal contour of the nose may be restored. The spongy tissue is very insensitive, so that a small amount of eucain or cocain is sufficient. Hemorrhage is free, but may be controlled by pressure and ligatures. Although these patients are usually plethoric and stand very well the loss of blood, it may be advisable to remove only a potion of the growth at one sitting. This plan has the further advantage of enabling the surgeon to observe the effect of a partialremoval of the tumor before completing the task. Removal may be effected in such a way that pedicled flaps are utilized to cover the raw spaces. Their vitality is low, and unless the pedicle is very broad, they are likely to slough. Therefore it is advisable not to undermine them too extensively. The results of this plastic surgery are very satisfactory (Figs 44 and 45). In some cases, if the quality of the skin is too poor, it is better to shave off all of the tissue down to the cartilage and to cover the wound with skin grafts.
Medical treatment through the years has included avoidance of stimulation factors (ie alcohol), appropriate cleanliness, and treatment of secondary infection and inflammation with antibiotics and steroids. In the 1920’s, treatment of the condition included X-ray and radium. Unfortunately, this was found to lead to a greater incidence of skin cancer and thyroid tumors 20 years later.
Surgical treatment has greatly benefited from the addition of lasers. Between 1908 and now, not only were scalpel used to “debulk” the tissue, but so have cryosurgical techniques, chemical peels, dermabrasion, the Shaw knife (a thermally heated scalpel), the Bovie, hot wire loops, and lasers.
The removal of the tissue is often referred to as “decortication.” The goal is to remove the tissue in layers and to avoid injury to the underlying cartilage. If 2-3 mm of skin tissue is left above the cartilage level, the nose regains its shape and there should remain enough sebaceous glands elements for re-epithelialize of the nose. A major advantage of the laser is the near bloodless field.
There is a beautiful example of the results obtained by use of the laser for treatment of rhinophyma here.
REFERENCES
Rhinophyma (Grand Rounds presentation at Baylor College of Medicine) by Randall S. Zane, MD; October 29, 1992 Diagnosis and Treatment of Rosacea; MedScape Article, May 21, 2002; Aaron F. Cohen, MD, Jeffrey D. Tiemstra, MD
















 Flowers, fox, rabbit, butterfly, flowers, frog, angel ….
Flowers, fox, rabbit, butterfly, flowers, frog, angel …. 





